THE BIG READ: As population ages, more are confronting the last taboo
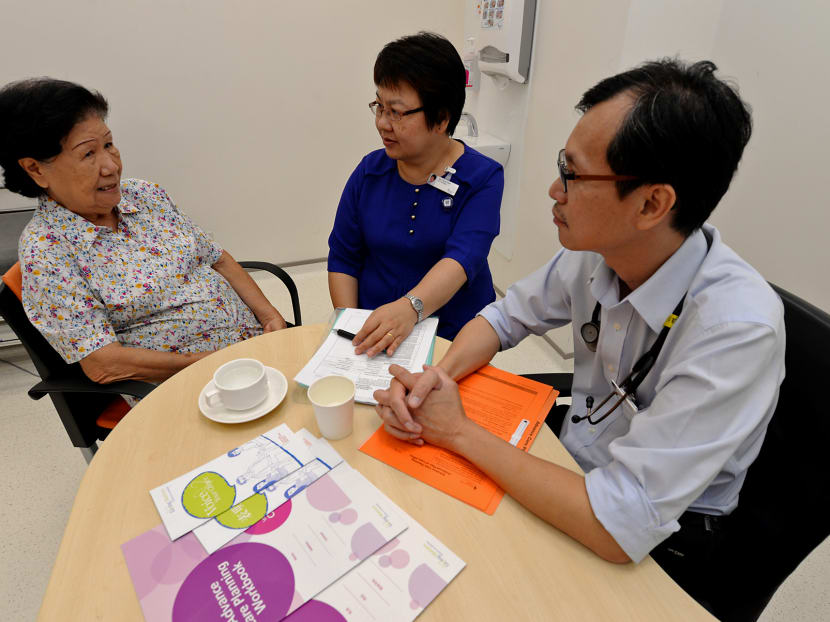
, 83, discussing death and care plans with Advance Care Planning Facilitator Ms Tan Seng Wah (Centre) and Dr Siew Chee Weng (Right), Department of Geriatric Medicine Khoo Teck Puat Hospital. Photo: Robin Choo")
Madam Eunice Ang (Left), 83, discussing death and care plans with Advance Care Planning Facilitator Ms Tan Seng Wah (Centre) and Dr Siew Chee Weng (Right), Department of Geriatric Medicine Khoo Teck Puat Hospital. Photo: Robin Choo

SINGAPORE — A third and more devastating stroke left retiree Madam Chan’s father-in-law bedridden in a nursing home for more than a decade, incapable of eating, speaking or moving. While it has been 15 years since her father-in-law died, Mdm Chan, 61, remains shaken by the memories of his ordeal, so much so that she has made clear to her family how she wishes to be cared for in her final days.
“All the children felt bad. Should we have revived him in the first place or let him go when he had the stroke? It affected all of us and we said we wouldn’t go through the same thing,” said Mdm Chan, who declined to share her full name. "Even if you have a special nurse or a private room, so what? You cannot talk or move. The quality of life (isn’t there).”
Via an Advance Care Planning (ACP) document, Mdm Chan, who has diabetes, has stated in black-and-white her wishes: “I’ve decided not to have artificial life-sustaining treatment and not to have CPR (cardiopulmonary resuscitation) if I have less than a 50 per cent chance of living. Between receiving care at home and in a nursing home, I chose a nursing home because it has facilities and trained personnel.”
Under the guidance of a facilitator at the Society of Sheng Hong Welfare Services, she has also appointed her husband as her substitute decision-maker.
The process of drafting an ACP document consists of a series of voluntary discussions on end-of-life care arrangements involving the individual, his loved ones, healthcare providers and a trained facilitator.
The document makes things easier for family members, said retiree Eunice Ang, 84, who did the ACP last year. “I prompted my late husband to do his too. I told him it’s good because we won’t feel guilty later. We do not know exactly what others wish for, so it’s best that they make their own choice,” said Mdm Ang, whose husband died of cancer in 2012.
Apart from the ACP, there are also the Advance Medical Directive (AMD) and Lasting Power of Attorney (LPA) that individuals can use to make decisions regarding end-of-life arrangements. An AMD, likened to a living will, is a document stating an individual’s wish not to have extraordinary life-sustaining treatment if he becomes terminally ill or unconscious. The LPA allows an individual to appoint trusted persons to make wide-ranging personal and financial decisions on his behalf if he loses his mental capacity.
Official statistics show a sharp spike in the take-up rate of these services. Since 2011, the Agency for Integrated Care (AIC) has seen 2,026 ACP discussions take place, with more than half (1,169) occurring in the past year. Over 2,000 AMDs were signed last year, more than the 1,800 made in 2013. As at the end of last year, the Ministry of Health (MOH) has more than 20,000 directives in its records.
Last year, more than 3,000 applications for LPA were given the green light by the Office of Public Guardian — about a third of the total number of applications were approved since 2010. Unlike the AMD and the LPA, the ACP document is not legally binding and it can cover funeral arrangements, for example.

“It’s more flexible and you can change your mind,” Mdm Chan said.
ACP was piloted in Tan Tock Seng Hospital in 2009. Two years later, MOH appointed the AIC to oversee and coordinate the implementation of a national ACP programme with public hospitals and community care providers. In the past five years, 1,400 ACP facilitators have been trained, with over a third (528) receiving training last year. Facilitators include doctors, nurses, counsellors, medical social workers and administrative personnel — most of whom are based in public hospitals.
“The training focuses on developing communication and facilitation skills, as well as an understanding of how the ACP framework works. Participants learn to guide patients and their loved ones through key components of the framework, including what it means for the patient to live well and meaningfully,” said Dr Irwin Chung, AIC’s deputy chief (care integration division).
Among an ageing population, death is, however, still a topic that is taboo for many.
Often, family members find it painful to broach the topic with their ailing loved ones, said Mr Andy Sim, a senior medical social worker at Singapore General Hospital. “They see it as taking away hope,” he said.
Mr Pak Chuan Poh, 88, was diagnosed with lung cancer last July. Since then, he has been receiving home palliative care from HCA Hospice Care.
Doctors have asked his children on their plans, should his condition turn critical. But to avoid upsetting their father, Mr Pak’s five children have decided against discussing the matter.
“The doctor did speak to my sister about this — for example, what happens if my father doesn’t wake up one day. But we haven’t made that decision yet,” said his son Hock Cai, 52. “We don’t dare to discuss these with my father. We want to let him be happy, and not be troubled by these things.”
Starting a conversation about death is often a thorny issue between family members, and even more so for doctors and medical social workers.
Medical social worker Venus Ther said: “It’s not a one-off discussion. It’s a process of building rapport, basic comfort and trust, because you’re talking about life and death. You need the groundwork.”
At the National University Hospital, on average, three in four referrals for ACP will give it a shot. Of these, about two-thirds complete the process.
As Dr Noreen Chan, a senior consultant at the National University Cancer Institute, put it, confronting one’s mortality is never easy. “Some patients are worried that if they complete an ACP, when they do fall seriously ill, they might not be treated at all,” she said. “This is not true. ACP is a means to think through and voice out one’s values and preferences.”
Dr James Low, a senior consultant at Khoo Teck Puat Hospital’s geriatric medicine department, noted how dogged attempts at broaching the topic could rub patients and their families the wrong way. “The patient might think you want him or her to die to save costs. But at the end of the day, the key thing is to save them unnecessary pain or suffering,” he said.
Still, healthcare professionals stressed the importance of planning for quality care during one’s final days. “When people are very ill and are unable to say what they want, it’s the family’s call,” said Dr Chan. “But if you as a patient never had a chance to discuss what you wanted, that leaves family members in a very stressful position. They’ll be wondering if they made the right decision.”
A recent study by the Lien Centre for Palliative Care (LCPC) and the National Cancer Centre found that patients with end-stage cancer are more willing to fork out money so they can die at home or avoid severe pain, rather than paying to extend their life by one year.
In contrast, their caregivers were three times more willing to pay to extend life by one year. The difference in patients’ and caregivers’ willingness to pay suggests the need to ask patients about their preferences directly when making decisions on treatment, as opposed to relying on input from caregivers, LCPC’s Assistant Professor Chetna Malhotra had said.
Healthcare professionals said that typically, two groups of people are inclined to do early planning: Those with chronic or terminal illnesses, and those who had recently lost loved ones.
Mr Tejas Ewing, 35, who runs his own business, intends to document his end-of-life care preferences, after losing his father last October following a protracted battle with cancer. His father, who died at 69, was in home palliative care for 18 months. During this period, although his father talked about his general wishes, he did not get to document his final-stage care preferences, Mr Ewing said.

“The reality is that it’s always going to be hard to have those conversations when the person is already sick — because nobody wants to think about every little detail and fill in forms about end-of-life once they’re already ill,” he said. “But it affects everything about your treatment: The kind of medication and ventilation they put you on, what they will do if you have a cardiac arrest, and all those things.”
He added: “It just so happened that my dad was lucid and alert until the final two days of his life. And then he went into a coma and died in his sleep.”
Mdm Chan recalled how her four siblings were divided over the funeral arrangement when their mother died. Some wanted a funeral service, while others wanted a cremation followed by a sea burial of the remains. “Those with the loudest voice win,” she said. After some wrangling, the siblings settled on a three-day service.
Dr Low noted that death could happen unexpectedly, and it is important for people to start discussions on end-of-life matters while they are younger, during middle-age, for example. “We should be discussing these things a bit earlier,” he said.
Palliative medicine pioneer Cynthia Goh noted how facilitators have a key role to play, and more training for this group is required.
“There is no template. Sometimes, we try to be efficient and look for targets and deliverables,” said Dr Goh, who is from the National Cancer Centre Singapore. Patients may feel pressured, and less inclined to open up when they are presented with a form to fill up, she noted. “People speak about (planning for end-of-life arrangements) in different ways,” said Dr Goh. “It’s not something that ends after signing the form.”
Stay in the know. Anytime. Anywhere.

Subscribe to our newsletter for the top features, insights and must reads delivered straight to your inbox.
By clicking subscribe, I agree for my personal data to be used to send me TODAY newsletters, promotional offers and for research and analysis.





